Situation report
To summarize the current state of the COVID-19 pandemic (CDC, 2021)(HHD, 2021):
1. There is a clear population divide between those vaccinated and those unvaccinated. In an example of a major city, 53% are fully vaccinated while 47% are unvaccinated. Among the vaccinated, there are 6% more with the first dose but not the second (59% at least partially vaccinated versus 41% unvaccinated). The highest rates of vaccinations are among the 60+ (90% fully vaccinated, 99% partially vaccinated, and 1% unvaccinated).
2. The difference between the infection rates from July 2020 (~21% in an example of a major city) and July 2021 (<5%, but with few consistently coming for testing) is from vaccinations and exposure prevention (source control, capacity limits, social distance, air circulation, barriers, hand hygiene, surface disinfection and/or PPE and respirators).
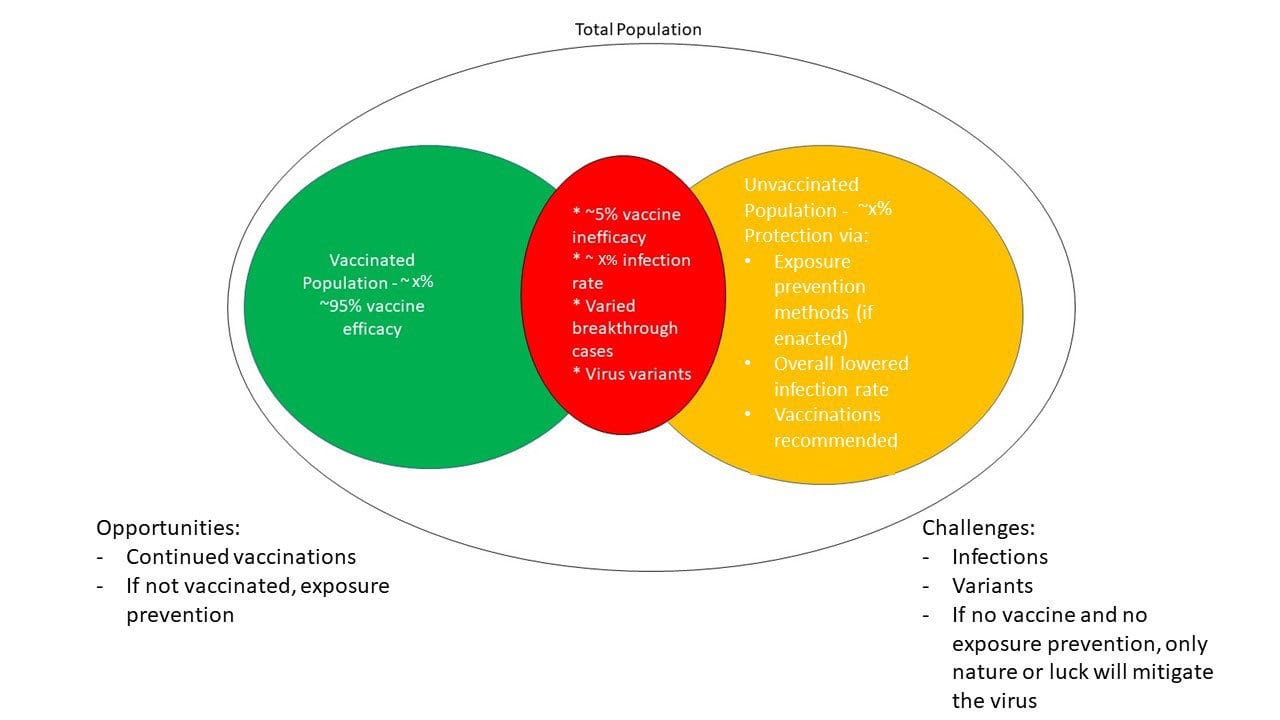
3. The current infection rate is <5%, but this is with few coming for testing. This means most known cases are severe enough for hospitalization. Most cases are unvaccinated. ~10% are the Delta variant, but the available vaccines are known to be effective against the COVID-19 variants. Outbreaks are still occurring among the unvaccinated. The ~5% vaccine inefficacy risk also presents a small risk of transmission. Infection numbers increased in all 50 states lately.
4. In short, vaccinations provide a good level of protection and COVID 19 is still circulating, mainly affecting the unvaccinated. If unvaccinated, exposure prevention methods such as social distance, avoiding large indoor crowds, and hand hygiene are good for preventing infections until the hazard and risk reduce. Face masks only serve for droplet containment (source control) that helps others (unvaccinated or the ~5% vaccine inefficacy risk). If unvaccinated and not enacting exposure prevention, the risk is around 1 in 20 or lower and with possibly heightened severity.
5. The key to risk reduction is to reduce frequency and severity. Frequency is reduced through vaccinations or exposure prevention (the fewer vulnerable hosts and the fewer infections and exposures, the virus stops circulating). Severity is reduced through vaccinations and medical treatment.
6. Without vaccinations or exposure prevention, the virus keeps circulating and will only stop through nature or luck. If it keeps circulating, the unvaccinated (especially without exposure prevention) and the ~5% vaccine inefficacy risk are at risk.
The risk assessment
As the Center for Disease Control (CDC) announced new guidance in May 2021 that those with complete COVID-19 vaccinations may begin relaxing exposure prevention protocols, the occasion could have been interpreted as a milestone in the then-20-month trajectory of the global COVID-19 pandemic, a victory of sorts. However, two factors prevented this from being the victory it should have been:
1. A significant percentage of the population is not vaccinated as of July 2021, even with vaccines available to them. This is not to judge anyone for not being vaccinated; there are many reasons why some are not vaccinated. However, the reality is that, without a vaccination, the risks of COVID-19 infections and further outbreaks are higher.
2. COVID-19 infections are still occurring and, among them, variants such as the Delta Variant are being transmitted; the risk of COVID-19 exposures is not currently low enough that the virus is not circulating among those without vaccinations.
This is important because, with COVID-19 infections still occurring and variants being identified, there is a need for exposure prevention. In analyzing risks, risk levels are only lowered by decreases in the frequency of exposure and the severity of the hazard; risk are not lowered by decreases in incidents resulting from the hazard. For example, when driving a motor vehicle on the freeway at 60 miles per hour, a high risk of a motor vehicle collision exists warranting the use of a seatbelt and defensive driving techniques. Even if a motor vehicle collision has not occurred in a time, this absence of an incident does not remove the risk from driving a motor vehicle at high speeds, so the risk controls (seatbelt and defensive driving) are still necessary. The only way to remove the need for the risk controls is to remove the risk, which means not driving the motor vehicle. With COVID-19, with the virus still existing at variable levels, to lower the actual risk, the virus’s presence needs to be lessened; this is done with vaccinations and/or exposure prevention. However, if vaccines are refused and exposure prevention methods are not enacted, the risk level remains and, if infections still occur, the virus can continue circulating.